Endocrinology and Hormonal Disorders
Foundations, First Signals, and Thyroid Reality Hormonal problems rarely announce themselves clearly. In real clinical practice, they tend to surface slowly and unevenly.
Free written quote from a NexWell coordinator, usually within 24 hours.
Quick answer
Foundations, First Signals, and Thyroid Reality Hormonal problems rarely announce themselves clearly. In real clinical practice, they tend to surface slowly and unevenly.
Endocrinology and Hormonal Disorders in Turkey
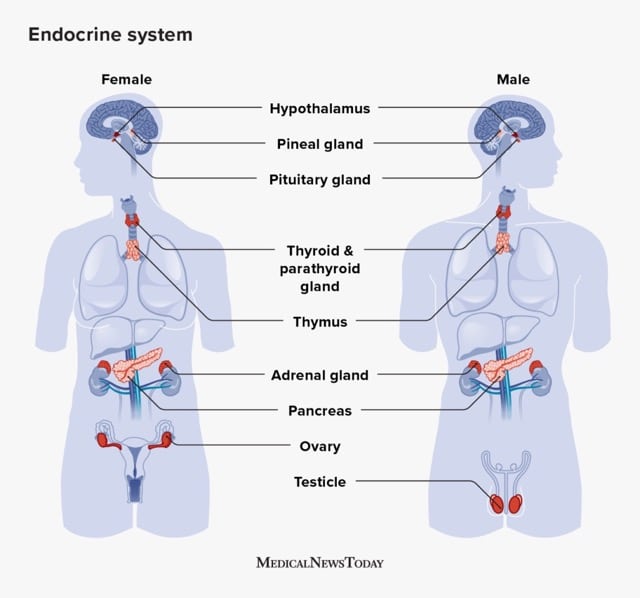
Endocrinology focuses on the diagnosis and treatment of conditions affecting the endocrine system, a complex network of glands and hormones that regulate many body functions. Turkey has emerged as a sought-after destination for endocrinology care, offering advanced medical facilities and expertise at competitive costs.
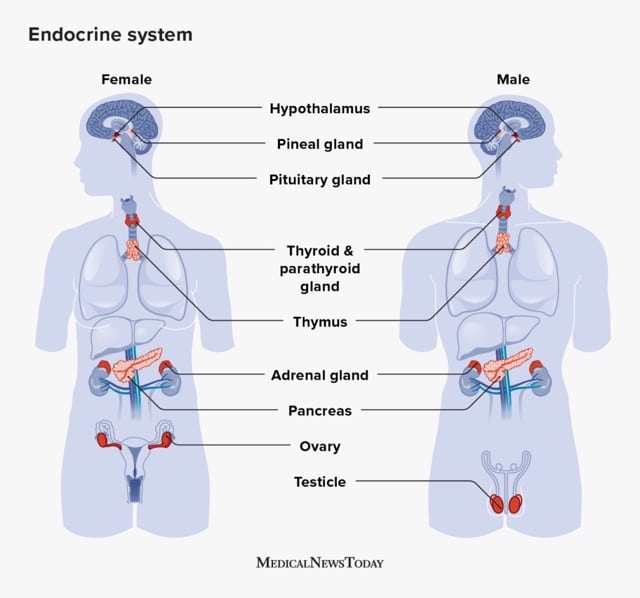
What Are Endocrine and Hormonal Disorders?
Endocrine disorders occur when the glands produce too much or too little of a hormone. These imbalances can lead to a wide range of health problems, such as:
- Diabetes Mellitus: A chronic condition affecting blood sugar regulation.
- Thyroid Disorders: Hyperthyroidism or hypothyroidism due to hormonal imbalance.
- Polycystic Ovary Syndrome (PCOS): A hormonal disorder in women affecting fertility and metabolism.
- Adrenal Disorders: Such as Cushing's syndrome or Addison's disease.
- Pituitary Gland Disorders: Affecting growth, metabolism, and reproduction.
Symptoms of Hormonal Disorders
| Common symptoms include: | • Weight fluctuations (gain or loss) | • Fatigue or energy changes |
|---|---|---|
| • Irregular menstrual cycles | • Hair loss or excessive hair growth | • Mood swings or depression |
| • Increased thirst or frequent urination | • Changes in blood pressure | If left untreated, these disorders can lead to serious health complications. |
Highly Skilled Endocrinologists
Turkey is home to specialists trained in diagnosing and treating a variety of endocrine disorders. Many physicians hold international certifications and have extensive experience with advanced diagnostic tools and treatment methods.
State-of-the-Art Facilities
Hospitals and clinics in Turkey are equipped with cutting-edge technology, such as:
- Advanced imaging systems
- Laboratory facilities for accurate diagnostics
- Minimally invasive surgical techniques
Comprehensive Medical Packages
Patients traveling to Turkey for endocrine care can benefit from all-inclusive packages that often include:
- Pre-consultation and diagnostic tests
- Treatment or surgery
- Accommodation and transportation
- Post-treatment care
Free Treatment Plan
Ready for a written Endocrinology and Hormonal Disorders quote?
A NexWell coordinator reviews your case and replies with a personalised treatment plan and indicative pricing — usually within 24 hours.
Common Treatments for Endocrine Disorders
- Hormone Replacement Therapy (HRT): Used to restore normal hormone levels in conditions like hypothyroidism or menopause.
- Diabetes Management: - Insulin therapy
- Blood sugar monitoring
- Lifestyle coaching
- Surgical Interventions: - Removal of tumors from glands (e.g., thyroidectomy, adrenalectomy).
- Minimally invasive techniques for faster recovery.
- Medications: Tailored drug therapies for hormone regulation and symptom management.
- Fertility Treatments: For patients with PCOS or other reproductive hormonal disorders.
How NexWell Supports Your Treatment Journey
NexWell collaborates with top endocrinologists and clinics across Turkey, ensuring a seamless experience for international patients. From consultation to post-treatment follow-ups, NexWell’s team ensures every step of your journey is handled with care.
Cost of Endocrinology Treatment in Turkey
Endocrinology treatment costs in Turkey are up to 60% lower than in Western countries. The average cost varies based on the treatment type and duration.
Price Comparison :
- Turkey: Starting at $2,000
- USA: $5,000+
- UK: €5,750+
- Australia: AUD 6,000+
How Do I Know If I Have a Hormonal Disorder?
Symptoms such as unexplained weight changes, fatigue, or irregular cycles are common signs. Consult an endocrinologist for accurate diagnosis.
Is Treatment for Endocrine Disorders Permanent?
Some conditions like diabetes require lifelong management, while others may be resolved with treatment or surgery.
Are Treatments Safe in Turkey?
Yes, Turkey adheres to strict international healthcare standards, ensuring patient safety and satisfaction.
How Long Does Recovery Take?
Recovery time varies based on the procedure but generally ranges from a few days (medication-based) to a few weeks (surgical).
Why NexWell for Endocrinology Care?
- Trusted Network: Collaborations with leading hospitals and specialists.
- Personalized Packages: Tailored care plans including diagnosis, treatment, and aftercare.
- Cost-Effective: Premium care at a fraction of the cost.
- Comprehensive Support: Assistance with travel, accommodations, and translations.
External Resources
- World Health Organization – Endocrine Disorders Overview
- American Diabetes Association
- Endocrine Society – Hormonal Health
Internal Links
- Explore Advanced Medical Treatments in Turkey
- Learn About Hormone Replacement Therapy
- Discover PCOS Treatment Options
Vetted partner network
NexWell coordinates with TEMOS-accredited clinics or Ministry of Health–licensed facilities in Turkey.
Free · No obligation
Get your free Endocrinology and Hormonal Disorders plan
Send your case and a coordinator returns a written plan and an indicative quote — usually within a day.
Related reading

Treatment Guide
Teeth Grinding and Bruxism: Causes, Damage and Treatment
Sleep vs awake grinding, causes and signs, damage to enamel and restorations, and night guard, Botox and protective treatment.
Treatment Guide
Sensitive Teeth: Causes and How to Get Relief
Why exposed dentin causes sensitivity, common triggers, at-home relief, and when sensitivity signals a problem needing a dentist.
Treatment Guide
Gum Recession: Causes, Treatment and Gum Grafting
Why gums recede, why it matters for sensitivity, decay and tooth loss, and what scaling, gum grafting and restoration can do.
Treatment Guide
Tooth Enamel: Why It Matters and How to Protect It
What enamel is and does, why acid and wear erode it, why it cannot regrow, and how to protect it.

dental
Dental Implants in Turkey
Replace a single tooth or your entire smile with premium dental implants in Istanbul. Same brands as London specialists, a fraction of the cost. 5-day treatment packages. TEMOS-accredited dental clinics.

plastic-surgery
Rhinoplasty Turkey Cost 2026: Open, Closed & Revision Prices
A buyer-focused cost guide for rhinoplasty in Turkey, covering open, closed and revision pricing with package evaluation criteria.
Plan the next step clearly
Use this page as a decision-support guide, then move into quote review, treatment comparison, and travel planning with coordinator support.
Decision Context
Patients compare this treatment inside the trip around it
Treatment pages perform better when they acknowledge arrival flow, destination trust, and the recovery rhythm patients are trying to visualise before booking.

The provider decision starts with arrival confidence
Patients compare treatment pages while also asking how first-day logistics, transfers, and scheduling will actually work.

The destination still influences medical trust
A treatment page is stronger when it recognises that the city itself remains part of the decision frame for international patients.

Recovery pacing changes how people evaluate options
Different procedures feel more or less realistic depending on how patients picture the slower hours between appointments.